Introduction
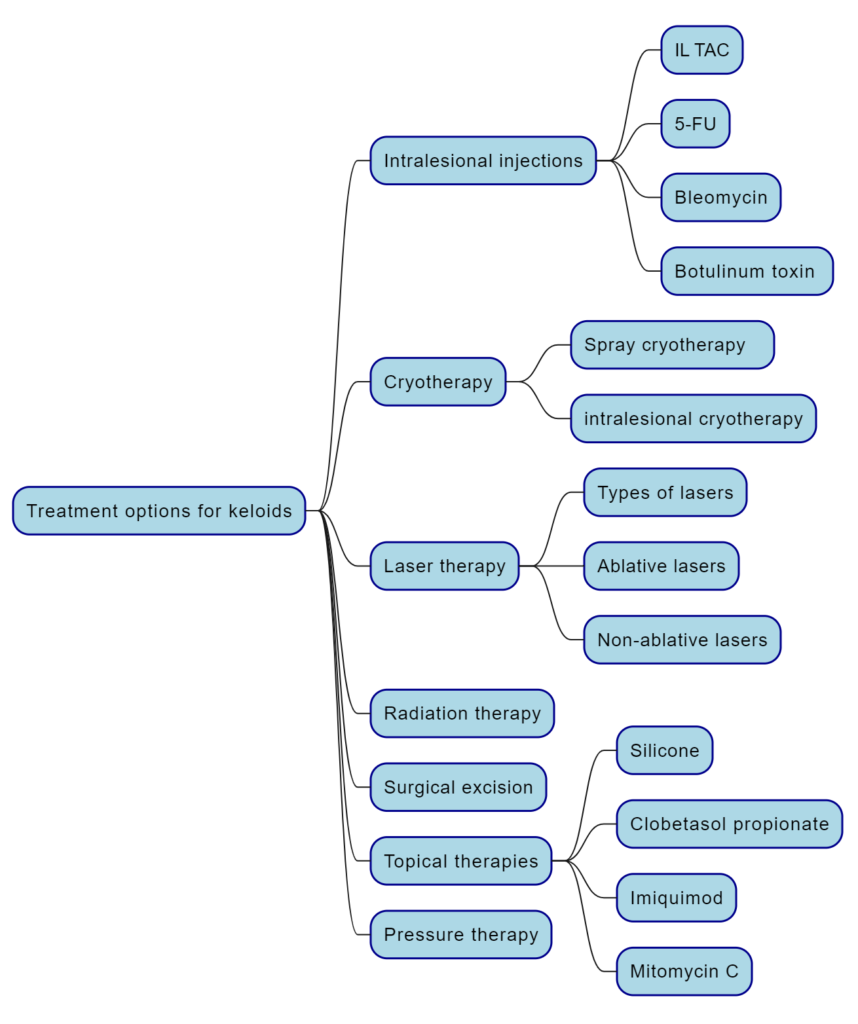
Keloids, fibrous tissue proliferations in the dermis, commonly result from cutaneous injury and disproportionately affect individuals with darker skin tones. These raised, firm lesions extend beyond the original injury site, causing significant functional and cosmetic burdens. Etiological factors include genetic predisposition, hormonal influences, and increased wound tension. Keloids are frequently pruritic or painful and can restrict normal movement by introducing tension in adjacent tissues. Keloid treatment options vary and may include intralesional injections, cryotherapy, laser therapy, radiation therapy, surgical excision, topical therapies, and pressure therapy.
Treatment options for keloids
- Intralesional injections.
- Cryotherapy.
- Laser therapy.
- Radiation therapy
- Surgical excision.
- Topical therapies
- Pressure therapy.
Intralesional injections
Intralesional corticosteroids for keloid treatment
- Intralesional triamcinolone acetonide (IL TAC) is the most common and effective corticosteroid for keloids. It can reduce keloid volume, height, and symptoms such as pain and itchiness. The dosage, frequency, and duration of IL TAC vary depending on the study and the keloid characteristics.
- Combination therapies with IL TAC and other modalities such as cryotherapy, radiofrequency, microneedle arrays, or surgical excision can enhance the outcomes and reduce the recurrence rates of keloids. However, the optimal combination and regimen are still unclear and need further research.
- Adverse effects of corticosteroids include skin atrophy, telangiectasia, hypopigmentation, ulceration, infection, and menstrual disorders. These effects may depend on the dose, route, and duration of corticosteroid administration.
- Dosage: The most common dosage is 20-40 mg/ml, but lower dosages may also be effective and have fewer adverse effects. The maximum dose per session of intralesional corticosteroid for keloids varies from 20 mg to 80 mg, depending on the keloid characteristics. Higher doses may be associated with systemic complications including Cushing’s syndrome.
- Frequency: The frequency ranges from single injections to weekly and monthly injections. The optimal frequency may be every 2 weeks, but more studies are needed to confirm this.
- Duration: The duration depends on the response and the type of keloid. Some studies suggest that 4-6 sessions are sufficient, while others continue until complete flattening or no response.
Intralesional FU for keloid treatment
- 5-FU inhibits fibroblast proliferation by disrupting DNA replication. It is used alone or combined with other treatments, often IL TAC.
- Combination 5-FU 50 mg/ml (0.9 ml) + 40 mg/ml TAC (0.1 ml) is more effective at reducing keloid height and improving Vancouver Scar Scale (VSS) scores than either treatment alone.
- Adverse effects include pain, ulceration, infection, hyperpigmentation, hypopigmentation, and telangiectasia.
- Tattoo method
- Anesthetizing the lesions.
- Applying 1 ml of 50 mg/ml 5-FU solution to each centimeter area of the lesion.
- Making punctures in the skin using a 27-gauge needle.
- Reapplying 1 ml of 5-FU solution to the surface and covering it to enhance absorption.
Intralesional Bleomycin
- Bleomycin, an antineoplastic agent, induces necrosis of fibroblasts.
- Bleomycin’s effects also include reducing blood supply to keloid tissue, which helps alleviate symptoms such as redness, swelling, and pain associated with keloids.
- Patients receive six doses of monthly 1.5 IU/m of bleomycin.
- Bleomycin treatment resulted in a 50% reduction in the Patient and Observer Scar Assessment Scale (POSAS) score from baseline.
- Bleomycin did not surpass the effectiveness of intralesional Triamcinolone acetonide (IL TAC).
- Additionally, bleomycin treatment was associated with an elevated risk of bulla formation and ulceration compared to IL TAC.
Botulinum toxin type A
- Botulinum toxin A (BTA) is a neurotoxin known for its paralytic effects, potentially useful in keloid treatment due to its ability to reduce muscular tension at wound sites.
- Two double-blinded controlled trials found no significant difference between BTA and Triamcinolone acetonide (TAC) in keloid treatment.
- In a head-to-head comparison with 5-fluorouracil (5-FU), BTA demonstrated significantly greater flattening of keloids.
- When used in combination therapy with TAC, BTA significantly reduced keloid surface area compared to TAC or BTA alone.
Cryotherapy
- Liquid nitrogen cryotherapy is commonly used for treating skin lesions by lowering the temperature to form ice crystals, which leads to cell dehydration, denaturation, and necrosis, resulting in therapeutic effects.
- Spray cryotherapy and intralesional cryotherapy are two methods that differ in efficacy, number of sessions, and side effects.
- Intralesional cryotherapy seems to be more effective, especially with newer lesions, but also more painful.
- Cryotherapy can be combined with other modalities such as surgical excision, steroid injections, or platelet-rich plasma to improve the outcomes and prevent the recurrence of keloids.
- Anesthesia: Cryotherapy can also be used as a form of anesthesia to reduce the pain caused by steroid injections.
- Technique:
- Application of lidocaine cream.
- Wait for 30 minutes.
- Administer liquid nitrogen spray.
- Position the spray nozzle approximately 1–1.5 cm from the treatment site.
- Apply a single freeze-thaw cycle until complete freezing of the keloid is achieved (typically 3–5 seconds).
Laser therapy
Types of Lasers for Keloid Treatment:
- Ablative lasers: erbium (Er:YAG) laser and CO2 laser. They cause local tissue destruction by targeting the water chromophore.
- Non-ablative lasers: ND:YAG, diode lasers, and pulsed dye lasers (PDL). They target melanin and/or hemoglobin.
Use of Lasers:
- Lasers can be used as independent therapy for keloids or in combination with other therapeutics to assist in drug delivery and penetration.
Investigated Lasers:
- In a cohort of prospective studies, CO2 lasers were the most frequently investigated for keloid treatment, followed by erbium ablative lasers, ND:YAG, diode lasers, and pulsed dye lasers (PDL).
Radiation therapy
Types of Radiation for Keloid Treatment:
- Electron beams and photon beams are commonly used for treating keloid tissue nodules.
- High-energy electron beams precisely target the area, reducing redness and overgrowth of keloids.
- Photon radiation inhibits cell proliferation in keloid tissue, alleviating keloid hardening and overgrowth.
Beta Radiation Therapy:
- Beta radiation, a type of electron beam therapy, is commonly used for keloid treatment.
- Radiation therapy is not recommended for pregnant patients, children under 12, or for keloids in radiosensitive locations.
- Concerns about cancer development post-radiation therapy on keloid scars are rare based on available evidence.
- Interactions between beta particles and tissue, such as ionization and excitation, release energy, promoting keloid tissue repair and improvement through various mechanisms:
- Inhibiting collagen synthesis, reducing keloid hardness and protrusion.
- Facilitating collagen degradation, flattening and alleviating keloid tissue nodules.
- Exhibiting anti-inflammatory effects, alleviating inflammation and redness in keloid tissue nodules.
Side Effects
- Side effects include acute skin reactions like desquamation and pigmentation, while late complications may include scarring, atrophy, and necrosis.
- Strict control of dosage and irradiation area is crucial to minimize radiation risks, as beta radiation is a form of ionizing radiation that can cause irreversible damage to surrounding tissues and other body parts if administered improperly or at excessive dosages.
Surgical Excision for Keloids
- Surgical excision is a potential treatment option for mature keloids after failure of first-line therapies.
- However, as a monotherapy, it is associated with a recurrence rate of up to 100%.
- To reduce the risk of recurrence, combination treatment modalities are commonly employed.
Topical therapies
Silicone
- Silicone materials are considered the “gold standard” for treating keloid scars due to their occlusive and hydrating effects.
- Studies have shown up to 90% improvement in keloid scars with the use of silicone dressings, but complete resolution has not been achieved.
- Both silicone sheets and gels have demonstrated equivalent efficacy in treating keloids.
- Recommended usage includes wearing silicone sheets for 12–24 hours per day for 3–6 months, or applying silicone gels twice daily.
- While no serious side effects have been reported, folliculitis is a potential adverse effect, and cost is a disadvantage associated with most silicone products.
Imiquimod
- Imiquimod is an immune response modulator that acts as a Toll-like receptor agonist, increasing the production of pro-inflammatory cytokines and inducing the expression of apoptotic genes in keloid tissue.
- It is commonly used at a 5% concentration for treating warts, basal cell carcinoma, and actinic keratosis.
- Studies suggest that adjuvant therapy with imiquimod cream after keloid surgery may reduce recurrence rates, although its efficacy remains uncertain.
- Reported side effects include pain, hyperpigmentation, and local skin reactions like irritation, erythema, erosion, and crusting.
Mitomycin C
- Mitomycin C, derived from Streptomyces caespitosus, possesses antineoplastic and anti-proliferative properties.
- It functions by inhibiting the synthesis of DNA, RNA, and protein, as well as fibroblast proliferation, thereby preventing cell division and reducing scar formation.
Clobetasol propionate
- Clobetasol propionate 0.05% cream, when used under occlusion with silicone dressing, is comparably effective to intralesional triamcinolone for treating keloids.
- This treatment option presents fewer adverse effects, making it suitable for patients with a low pain threshold, needle phobia, or those who prefer home-based treatments.
- The combination of clobetasol propionate cream and silicone dressing offers a viable alternative for keloid management, providing effective results with reduced discomfort and inconvenience.
Pressure therapy
- Garment pressure therapy for keloids is effective within pressure ranges of 15 to 40 mm Hg, pressures exceeding 40 mm Hg may cause complications like maceration or necrosis.
- Constant pressure applied during scar maturation may limit blood, oxygen, and nutrient supply to scar tissue, controlling collagen synthesis and speeding up the natural maturation process.
- Patient-led solutions, such as adapting clothespin springs or using metal coins, have provided simple and safe alternative pressure garment methods.
- Garment pressure therapy should begin as soon as possible after wound closure.
- Worn for at least 23 hours/day to provide consistent pressure.
- Treatment duration varies – at least 6 months, up to 3 years recommended.
- Extended wear time and restriction of movement lead to discomfort and poor compliance.
Sources
- Intralesional Corticosteroid Administration in the Treatment of Keloids: A Scoping Review on Injection Methods.
- Keloid treatments: an evidence-based systematic review of recent advances.
- Diagnosis and Treatment of Keloid: Method Summary and Effect Evaluation.
- Management of keloid scars: noninvasive and invasive treatments.
- A Randomized, Single-Blind Trial of Clobetasol Propionate 0.05% Cream Under Silicone Dressing Occlusion Versus Intra-Lesional Triamcinolone for Treatment of Keloid
#intralesional corticosteroids #keloid #keloid treatment